In a relatively short period of time, the Western healthcare system will undergo structural and organisational upheaval caused by an ageing population, exponential growth in numbers of the chronically ill, technological advances, and a shortage of caregivers. One possible solution to this problem is the automation of medical work using artificial intelligence. But if the patient becomes the sole manager of their health, what happens to the other workers and stakeholders in the healthcare sector?
Healthcare by algorithm
It’s the year 2033, Michelle is 87. She lives alone in her apartment, which lies in a new residential building designed for the elderly in an affluent neighbourhood, 6 miles from Brussels. She loves to bake nice cakes for her great-grandchildren when they come to visit. She also loves chatting with them on the giant screen in her living room when they get home from school.
Michelle is part of the post-war baby-boomer generation. Now a ‘granny boomer’, she symbolises an ageing Europe. Throughout her life, Michelle has benefited from huge advances in medicine and has seen her life expectancy lengthened thanks to close medical and social care, which is costly in terms of both human and financial resources.
When Michelle took a fall three years ago after getting up in the night to go to the toilet, her petbot (everyone seems to have one of these cute algorithm-based robotic animals these days) sent an alert to the smartphones of her nearest and dearest (friends, family, and carers). The petbot generated a geolocalised call to the person nearest to Michelle’s home so they could come over and help her up. The petbot also alerted the emergency services.
The team supervising Michelle’s neighbourhood instantly received the information necessary to make a clinical decision: her pulse, heart regularity, blood sugar level, temperature, level of consciousness, and medical history. The primary care team waited for visual contact with the person who went to help Michelle in her home. Thanks to the data provided by this person via the petbot’s communication interface, the algorithm was able to decide that medical assistance was not necessary.
So, thanks to the automated environment provided by her insurer, Michelle didn’t spend the whole night on the floor waiting for help, she was not discovered at noon the next day when her carer came to help her make lunch; Michelle didn’t panic and call an ambulance, and didn’t spend five days in hospital under observation because she had spent nine hours on the cold floor of her bedroom.

Remote monitoring of her vital signs isn’t the only technology that Michelle benefits from. Without even having to use a smartphone or a complicated piece of software, Michelle receives an optimal level of care. Her blood pressure is monitored each week via a discreet bracelet. Her petbot records information and sends it monthly to the primary care team. The nurse keeps in regular video contact with Michelle to update her on changes to treatment, and no longer needs to visit her frequently to measure her health parameters or check she’s taking her medication.
As far as medication is concerned, the artificial intelligence included in the petbot also calculates any changes in dose necessary based on the parameters measured and recorded, and suggests them to the doctor in the primary care team.
When the doctor approves a change in medication, the prescription is sent directly to the robot in the local pharmaceutical centre, which manufactures the pills using 3D technology so they are completely tailored to Michelle, and also contain the three other drugs that she must take daily. The new box of pills is delivered to her home the next day by drone, and Michelle confirms receipt with a finger print or through facial recognition. She puts the pills in her petbot, which instantly notifies the doctor that the new course of treatment has started. When authorised by Michelle, her friends and family are also informed of the changes made to her treatment programme. Thanks to her petbot, Michelle never forgets to take her pills.
Thanks to the automated environment provided by her insurer, Michelle didn’t spend the whole night on the floor waiting for help
Her Uber Health subscription lets Michelle schedule trips to the hospital for tests; she no longer has to ask her daughter to take her. Her smart fridge sends an automatically generated shopping list to the local distribution centre. When she has to do physiotherapy exercises to rehabilitate the shoulder that she injured in a fall, Michelle uses virtual drumsticks to play music controlled by the motion sensor built into the camera of the TV in her living room.
Eventually, Michelle is able to stop taking pills to help her sleep and no longer risks falling in the night due to their side effects. Every night, Michelle’s petbot launches a programme to help her sleep, with music, a soothing voice, and comforting colours. Michelle is no longer anxious because she knows that her petbot will watch over her at night and warn those close to her if there’s a problem.
For every aspect of Michelle’s health – physical, psychological, and social – there is an automated care solution.
An ageing healthcare system
Today, almost 20 per cent of Europe’s population is over the age of 65. But often overlooked is that an ageing Europe goes hand in hand with a sick and dependent Europe, because longevity is not associated with a reduction in ill health. While medical advances have allowed us to extend the lives of the chronically ill, they have not enabled us to completely cure them.
Demographic forecasts are telling: the proportion of Europeans aged 65 or over will double between 2010 and 2050, while the proportion of those over 80 will double by 2080, from roughly 6 per cent today to 12 per cent. Dependence levels will grow too, [1] from almost 30 per cent now to 50 per cent in 2080. Furthermore, it is estimated that 60 per cent of the European population will be obese by 2050, with current levels of obesity three times those of 1980. Cases of cancers and diabetes will also follow this trend.
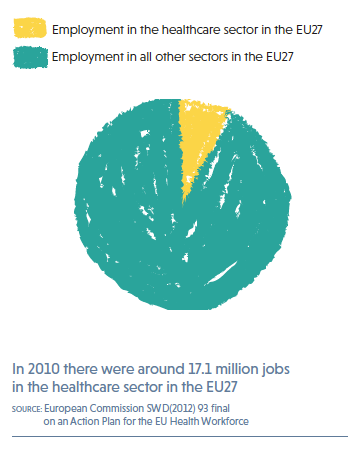
As Europe ages, the Europeans that care for its population are ageing too. In 2009, 30 per cent of European doctors were aged over 55. These doctors are now nearing 65 or so, and most are at the end of their careers. Yet healthcare is one of the largest sectors of Europe’s economy, employing almost 17 million people and accounting for 8 per cent of all jobs[2]. It faces three major challenges. There are not enough new entrants to the workforce to replace those retiring. The psychological conditions particular to this type of work result in a quick turnover. And new technologies require advanced and continuous training across the whole sector.
While medical advances have allowed us to extend the lives of the chronically ill, they have not enabled us to completely cure them.
The health policies adopted by European states fail to provide an adequate response. On the one hand, there is a lack of investment in prevention to halt the growth in chronic disease and, on the other, mechanisms that limit the numbers of healthcare professionals persist (through the restructuring and merger of healthcare organisations or the restriction of access to medical and paramedical degrees seen since the 1990s).
While the period between 1960 and 1990 saw the number of doctors triple in most OECD members (except the United Kingdom and Japan) leading to an abundance in certain countries (Greece, Spain, Italy, and Belgium), numbers have stagnated since the 1990s and no longer seem sufficient to meet long-term needs. Despite the clear lack of scientific evidence justifying the setting of quotas to regulate the use of healthcare, limited access to the medical profession through quotas remains the norm in Europe.
Since April 1993, thanks to a European directive doctors have been able to move freely across the EU and mutual recognition of their qualifications has been facilitated. But free movement has lacked oversight and failed to take into account different levels of income or different healthcare structures in each EU Member State.
What’s more, any analysis of medical demographics in Europe is complicated by two main factors: differences in the organisation of public healthcare from one country to another, and the lack of a shared definition for healthcare professionals. For example, a general practitioner in Belgium does not have the same skills or functions in a healthcare organisation as a primary care provider in the UK or Ireland.
Despite the clear willingness to allow the free movement of healthcare professionals, health planning policy is one of the poor relations of European integration. Indeed, it is only since 2010 that some national professional bodies have started working together to improve the assessment of migratory flows and their impact on the functioning of health systems across Europe[4]. This apparent lack of political foresight and concerted action on health planning will, by accident or design, profoundly transform the organisation of healthcare.
What does the future hold for our health system?
Along with education, healthcare is one of the last areas in which automation and digitisation have yet to become widespread. New technology is ready to provide a seemingly personalised service in areas where human contact seems irreplaceable.
And while Europeans (patients and healthcare professionals) remain reluctant to use new healthcare technologies and share their health data, the generation that has grown up with smartphones in their hands will quickly change this situation. In the last five years alone, healthcare has been bombarded by new technologies. Private platforms for consulting doctors online have proliferated; connected devices that measure vital signs have become commonplace; health-monitoring and coaching mobile apps have exploded – with insurers and social security systems beginning to pay for certain apps – and states have implemented e-health plans to connect healthcare professionals and patients as part of wider e-government projects.
The economic and medical implications are enormous: not only is the pharmaceuticals and healthcare sector financially attractive – currently considered one of the most promising to invest in by financial markets, [3] with e-health having just been opened to private-sector competition – but it is a way of reducing healthcare costs. Mobile health applications were worth 25 billion dollars worldwide in 2017. A study published in The Lancet in November 2017 estimated that the widespread adoption of digital health applications for five types of patients (diabetes prevention, diabetes, asthma, cardiac rehabilitation, and pulmonary rehabilitation) could save the United States’ healthcare system 7 billion dollars a year. [4]
The end of the 20th century saw the traditional silos of healthcare organisation in industrialised countries begin to break down, with medical tasks shifting from doctors to paramedical personnel and doctor-nurse tandems becoming common. The 21st century will herald DNA repair, the replacement of medical expertise by algorithms, and health self-management by patients. The automated reading of health parameters will free doctors and nurses from a whole series of repetitive tasks. Patients will be empowered by e-learning, and chatbots (automated conversation programmes responding to keywords) will take over medical monitoring with the latest algorithms providing quality care that is scientifically proven.
New technology is ready to provide a seemingly personalised service in areas where human contact seems irreplaceable.
While the patient-caregiver relationship remains the cornerstone of the placebo effect (patients feeling they are being listened to and treated plays a key role in healing), studies show that users of mobile health apps feel they are better supported and listened to than in the current system where the doctors are forced to limit contact time when their workload is too large. [5]
Healthcare automation will not only save time in managing people’s health events, it will also lower the critical threshold of primary-care physicians necessary to meet our healthcare needs. We are facing a major shift in public health in terms of the treatment of health problems, prevention policies, and the organisation of healthcare systems.
As she gets older, Michelle will witness the transformation of whole swathes of medical specialties. Instead of a radiologist, an artificial intelligence programme will analyse her scan to check that her cancer is still in remission. When she needs insulin to control her diabetes, a device implanted in her stomach will automatically calculate the dose to deliver without the aid of a nephrologist. If Michelle has a car accident that damages her stomach, 3D printing of human tissues and organs will speed up the surgeon’s work. The health insurance that Michelle will have to take out will use precise risk reduction tools. And Michelle’s future great-grandchildren will benefit from genetic diagnostics and possibilities for early repair.
An inevitable reorganisation
Healthcare automation will bring with it a specific set of problems. Private databases of medical records carry the risk of breaches in medical confidentiality and open the door to greater commercialisation of medical data. With more algorithmic profiling (even if this is regulated by the new General Data Protection Regulation), educating and training people in self-management and the use of IT tools will be essential. Energy consumption will increase. Access to these new technologies will be a source of inequality, and cross-border and virtual consumption of healthcare will make public health policy difficult to organise and forecast at a national level.
The revolution in preventive and regenerative medicine brought about by innovations in genetics will profoundly change medical treatment and make curative medicine obsolete, so it is essential to quickly reform the training of caregivers. Rapidly modernising training is especially important as healthcare education and organisation are high-inertia systems that will not keep pace with the dynamism of the tech sector. In tomorrow’s world, we will have even greater need for doctors, but they will have to work alongside engineers and computer scientists to create and manage healthcare tools.
[1] The old-age-dependency ratio is the ratio of the number of elderly people at an age when they are generally economically inactive (i.e. aged 65 andover), compared to the number of people of working age (i.e. 15-64 years old).
[2] European Commission (2012). Commission Staff Working Document on an Action Plan for the EU Health Workforce. bit.ly/2qm4NiF
[3] Debbie Carlson (January 2018). The Best Stock Market Sectors in 2018. U.S. News. bit.ly/2qjOxiD
[4] Does Mobile Health Matter? The Lancet. Vol. 390. (Nov. 18, 2017) bit.ly/2EzMjAl
[5] Powell, Rhea E. et al. (May/June 2017). Patient Perceptions of Telehealth Primary Care Video Visits. Annals of Family Medicine. Vol. 15 no. 3 225-229.